Summit Partners’ misguided acquisition of Addiction Campuses, renamed to Vertava Health post acquisition, was indicative of a prevailing thesis around residential SUD treatment at the time. In less than 4 years, Summit had sold off all 4 of the residential facilities, had opened and closed a handful of de novo outpatient facilities, and then ended up rebranded as Blended Health with its primary holding of Connections Wellness, a series of teen outpatient facilities in Dallas, TX.
Mistakes were made in reading the macroeconomic trends in behavioral health, the implementation of an add-on growth strategy, and inaccurately recognizing growth drivers in the space. However, Summit Partners was far from singular in its mistakes, which is why this particular acquisition represents an excellent case study that can be extrapolated to the field as a whole.
Both strategic buyers and private equity-backed portfolio companies have mostly failed to deliver on the perceived potential within the SUD space. No organization providing residential SUD services exclusively to the commercially insured has succeeded in dominating the space nationwide, a core part of the underlying thesis for most firms making forays into the vertical.
In this analysis, we’ll look at macroenvironmental challenges, shifting trends, and operational assumptions that have served to undermine many investment theses in SUD treatment continuing through to today.
Macro Headwinds Buffeting Providers
At the time of Summit Partners’ acquisition of Addiction Campuses, the market was frothy, with valuations for some providers at 10 times earnings or more. Behavioral Health, and SUD in particular, were seen as markets with significant opportunity for expansion and which were also considered to be ripe for a traditional roll-up scenario.
However, firms investing in the late 2010s failed to recognize specific headwinds or did not properly evaluate their impact on acquisitions. This is understandable as the market dynamics were radically changing at the time.
From the period of roughly 2008 to 2017, the SUD market had been defined by high reimbursement out-of-network residential treatment, with patients flying from all over the country to seek care, an environment in which Addiction Campuses was well-suited. In contrast, by 2019, most patients were attending in-network facilities within driving distance of their homes and entering lower levels of care.
Addiction Campuses, set up in the heyday of high reimbursement destination treatment, was not well positioned for these new market dynamics.
The Shift from OON to INN
The bottom had started following out of the OON model as early as 2017, and we began to report on its end by 2018. The drop in revenue from this shift was substantial. An OON reimbursement rate could be as high as $3,000 per day, while an INN might average around $1,000. That’s a 66% loss in average daily reimbursement (ADR) revenue! Not only were reimbursements drastically reduced, but the length of stay was also under pressure. Providers used to getting 60 or even 90 days were now getting 30 days or less. This particularly impacted the marketing economics, as we’ll talk about shortly.
Having extensive experience in broader healthcare, Summit Partners likely recognized the shift from OON to INN reimbursement as evidenced by the newly rebranded Vertava Health’s move to in-network contracts fairly soon after the acquisition.
But they likely failed to understand how Vertava Health’s geographic positioning would be negatively impacted by the market’s move to in-network reimbursement. Each Vertava facility was 1-2 hours outside of a metropolitan area. The Ohio facility was situated on substantial acreage two hours outside of Cleveland, Cincinnati, and Columbus in the tiny town of Sherrodsville, OH (population 221).
While facing sizeable downward revenue pressure, Vertava Health's margins were further squeezed by high fixed real estate, maintenance, and staffing expenses. The large sums collected from OON reimbursements had been used to finance these costs. With the shift to lower in-network reimbursement, there was no way to comparably lower expenses.

Mortgage/lease and maintenance costs were fixed. Each Vertava facility had at least 100 beds on significant acreage. Additionally, licensed medical and behavioral health staff did not want to live in the middle of nowhere. To attract and retain talent, higher-than-average comp and benefit packages are required. Margins were squeezed between lowered reimbursements and uncompetitively high labor costs compared to their metropolitan competitors, which were springing up everywhere. These competitors weren’t buying luxury facilities with extensive acreage, and they were situated near metropolitan areas, so they had easy access to talent with no need to offer higher than market rate comp and benefit packages.
Increasing Urban Competition
The residential treatment industry had been founded on the fly-away model. This had originally occurred for two reasons.
- Since insurance didn’t cover it, few people could afford treatment, meaning a relative handful of providers served the entire country.
- The income bracket that could afford $3,000-a-day private pay treatment expected luxurious surroundings.
Not recognizing these driving forces, many providers (and their investors) assumed that destination treatment was preferred by patients and families. Often, a key underlying assumption was that a patient needed to “get out of their current environment.”
In reality, this was not the case. In fact, even back at this time, we saw in our data here at Circle Social that the majority of patients came from regional areas or, at the very least, followed the most convenient flight routes. For example, patients from New York or Philadelphia flew to Florida, but not to Denver or California. Patients from Portland would go to Orange County, CA or Prescott, AZ, but not Florida. As more and more providers started popping up in major cities across the country, patients and families frequently chose to go closer rather than farther away, usually within a distance of 70 miles or less.
One other factor of note here was cost. In the residential OON SUD heyday, most providers played fast and loose with “perks” such as covering the cost of airfare or conveniently ignoring the collection of deductibles. In this way, the monetary cost of treatment was non-existent for many patients.
By 2019, the reduction in revenue from dropping insurance reimbursements meant that providers could no longer afford to look the other way when it came to collecting patient responsibility, such as deductibles or co-pays. Paying for flights had also become economically untenable, and updated legislation (EKRA) made provider payment for flights illegal.
A final factor, though one that didn’t start having much impact until later, was that insurance companies were also promoting local care. We have strong relationships with several of the large payers. Relaying what they were seeing in their claims data, patients who received treatment closer to home were ultimately more successful in their recovery. This was because of better integration into local healthcare facilities, support of nearby family and friends, and ease of transition back into everyday life.
For all these reasons, if a patient or family had to choose between a treatment center located in their backyard versus one a two-hour drive, or a three-hour plane flight away, they went with the program closer to home.
We also have to remember that these faraway programs had historically served a wide geographic area, indicating that large facilities of 100 beds or more were not self-sustaining within a narrow geographic radius. Marketing efforts geared for vast geographic coverage on a fly-to-treatment model were not well-positioned for reputation-focused local healthcare marketing.
And it’s not just patients who prefer programs closer to home; referral partners are more likely to refer locally as well. After all, local providers are plugged into the community, having regular contact with referral partner staff through meetings, professional networking groups, conferences, and organically crossing paths for work-related tasks during their usual day-to-day. Nurses meet up with and talk to other nurses. Therapists meet up with and talk to other therapists.
When your entire staff lives and works in isolation 2 hours away, neither structured nor organic relationships readily form. Distance from metropolitan areas created a distinct disadvantage.
Marketing Costs Increase as Percentage of Revenue
With patients preferring to be closer to home, this meant that destination treatment providers had to pay significantly more in marketing costs. From our data, this was a rate of about 3:1. When patients and families were comparing options, they were 3 times more likely to choose a comparable local provider than one farther away (meaning marketing acquisition costs increased by the same rate as a factor of distance).
The OON destination model had relied primarily on three marketing channels:
- Google Ads
- Search Engine Optimization (SEO)
- Business Development Outreach
Google Ads are notoriously expensive in the addiction treatment space, having one of the highest cost-per-clicks in the world for high-intent treatment terms. It was not at all uncommon for a provider to pay $15,000 in Google Ads expense to acquire a patient. When providers were making $90,000 or more per patient, that expense was manageable. When providers were only making $30,000 per patient, not so much.
From our experience coming in and overhauling marketing for organizations like Vertava Health, we can tell you that internal teams and agencies at the time had no real understanding of how to optimize campaigns for the treatment space. Accounts were not set up properly, and little to no regular optimization occurred. Oftentimes, providers didn’t even know how much they were paying to acquire a patient because tracking wasn’t set up properly or it had never been set up at all!
The reality was that providers hadn’t had to worry about costs. As long as revenue was higher than expenses, little attention was paid to streamlining various elements of the organization, marketing being one of them.
For an acquirer performing due diligence, they might see a lot of inquiries coming in, but the organization itself had little to no insight on what was working or how much it cost.
To further complicate matters, while our professional account management during this period was able to reduce Google Ads costs by as much as 75% for providers, this was still too much for a provider to swallow at the new in-network reimbursement rates. Yet, historically, many providers had received a large percentage of admissions from Google Ads. This meant their primary acquisition channel, which they relied heavily on, was no longer viable as a primary channel. They rarely had a backup plan. Furthering the pain, unlike Google Ads, most marketing channels take months to build presence and move individuals through a decision-making cycle. Having not invested in these channels previously, the time and effort to do so was a major obstacle, with the most common result being providers choosing not to make the investments. Instead, providers doubled down on what had become ineffective strategies, hoping against hope they could make them work again, but only serving to further a downward financial spiral.
SEO and business development had different but related headwinds. From an SEO standpoint, most large providers across the country had developed a clandestine array of unbranded websites. The strategy here was two-fold. Google will only rank one page per website for a given term. By having additional websites, a provider could rank more than one site for the same term, both increasing their chances of getting an inquiry and preventing competitors from showing up in results.
Unbranded websites were also thought to convert better (we actually showed that this was not true after aggregating data across tens of millions of hits between the two site types, but our data wasn’t widespread knowledge at the time). An unbranded site was more likely to look like a non-profit or government help site, so it was thought to generate more inquiries than the branded sites.
Addiction Campuses, like most other providers, had had a number of these sites, most notably, rehabcenter.net. In 2017, such sites became a liability. Google implemented regulations stating that no entity owning unbranded websites would be allowed to advertise on Google. All addiction treatment providers were required to use a third party called LegitScript, which checked Whois and related ownership records to verify that unbranded websites weren’t being used.
In addition to Google’s regulations, the field as a whole had come to view unbranded sites as a deceptive, unethical marketing practice. Community partners were unwilling to refer to organizations using such tactics once discovered.
Not only was there pressure to drop high-ranking unbranded sites, but the Google algorithm itself was changing. Starting in 2015, Google began making significant updates to its algorithm targeting Your Money Your Life (YOLO) entities online. These initial forays were crude, but became more refined and sophisticated with each subsequent update. Healthcare and behavioral health providers fell under the Your Life portion of these updates. Google correctly recognized that its users were mostly looking for local healthcare providers. When the average patient wants to see a doctor, a counselor, a dentist, or enter a treatment program, they’re not looking for one halfway across the country.
To this end, Google started sorting results by local entities utilizing a verified Google My Business profile. Previously, it was possible to rank a website nationally, in any city in the country, by implementing SEO best practices on the pages. A provider with a physical location in Huntington Beach could rank pages across the country in Atlanta, Chicago, Asheville, wherever. This could be done both for location-specific pages and general treatment pages. In this sense, the best SEO won. Sites with better SEO dominated the search results nationally.
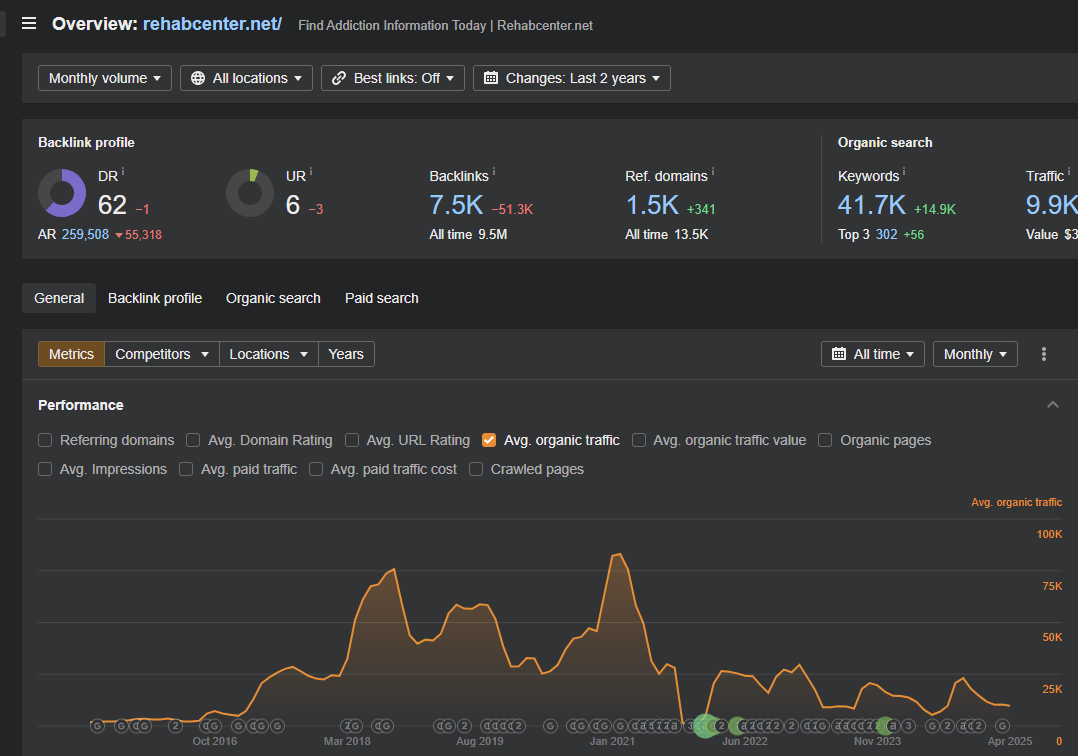
This all began to change in 2018. It took a couple of years for Google to really refine its ability to localize search rankings. Still, all the providers who had spent so much money and time ranking their sites nationally now saw dropping traffic and inquiries. Using standard SEO tools, below is an example from rehabcenter.net, previously an asset of Addiction Campus/Vertava Health (vertavahealth.com is now defunct and no longer has data available). We can see the constant downward trajectory of the site from 2018 to the present. There was a 3-month anomaly from Jan-March 2021, but such spikes occasionally happen during an algorithm tweak as result sets stabilize from various updates.
With SEO being the third leg of Vertava’s marketing stool, heavily reliant on national rankings for both rehabcenter.net and vertavahealth.com, this was a large blow to total inquiry volume.
Finally, there was business development. Up until this time, the work of business development was to engage in a practice we refer to as “horsetrading.” During this period, the market of SUD treatment was highly fragmented. Most providers, Addiction Campuses included, did not have a full continuum of care and were not in-network with most insurance providers. Those with more capital, built high-cost residentials. Those with less started low-cost IOPs. Those with more capital often invested in larger properties and stayed out of network, while those with less invested in more mundane facilities and went in-network.
What this created was a hodgepodge of different providers offering different levels of care or insurance involvement. Providers then effectively created extensive referral networks to refer patients between each other. While each provider was a distinct entity with different owners, they all ended up working together in these networks, in effect, pooling marketing dollars and resources, then trading patient inquiries amongst themselves.
In this way, the business development representative’s job was simply to identify mutually beneficial relationships, then go golfing, to the cigar bar, or grab coffee or lunch with reps from other programs. The conversations went something like this:
Rep 1: “We don’t take Cigna, but we take United. What about you?”
Rep 2: “Ok, we take Cigna but don’t take United. We’ll send you our United, and you can send us your Cigna.”
As you can see, there wasn’t much to this role. It was simply a matter of finding a reciprocal relationship, and it ended up being a bit of a popularity contest in the more competitive locations. With so many reps running around, those who could refer out the most, or the most likable reps, could cement stronger referral partnerships. Little was needed in terms of outreach expertise or even industry knowledge.
Nowadays, referrals come not from reciprocal relationships, but from other community partners, mostly in healthcare, such as hospitals or individual therapists. However, these providers care about different things. Rather than going golfing and discussing insurance policies, these partners want to know about the care model, about how the program ensures outcomes, and about care follow-up. These are conversations that the old generation of BD reps couldn’t have. Most BD reps had never even had training on the care model or seen it in action. Despite potentially a decade of experience in such roles, they were at a loss regarding the skills required to forge these new relationships.
With the move to in-network and the drop in reimbursement rates, providers cherry-picking which insurance to go in-network with and not offering multiple levels of care became unsustainable. Many providers still paid north of $5,000 in marketing expenses per admission. Turning away a patient because they didn’t offer that level of care or take their insurance became untenable. Additionally, providers now needed the extended revenue of a full continuum of care to stay afloat. Residentials needed the extended revenue from adding on PHP and IOP levels of care to absorb the excessive marketing costs.
At the time of Summit’s acquisition of Addiction Campuses, the three primary channels it had relied upon all came under fire for different reasons, resulting in severely diminished or cost-prohibitive inquiry volume. As we can tell you from direct experience, this was the situation for most providers of comparable size across the country at the time.
Missteps Post Acquisition
If these headwinds weren’t enough, Vertava Health also took several missteps that made things even worse.
What’s in a Brand Name?
First and foremost was the brand name change from Addiction Campuses to Vertava Health. The idea of a name change was smart. Addiction Campuses had developed a reputation for deceptive marketing practices and did not have the best name in the field. Since most SUD providers are reliant on about 70% of their patients coming from community referrals, having a good reputation is essential for sustainable success. Addiction Campuses had previously avoided this conundrum by relying on its massive investments in Google Ads and SEO, which then fed reciprocal referral volume for other SUD providers that were not as concerned about reputation.
With the aforementioned volume drops in both Google Ads and SEO, they no longer had reciprocal referral volume to horsetrade. On top of this, the deceptive or questionable practices of some providers in the SUD space were getting more and more media attention. This made it so that community referral partners started to become aware of these activities, decreasing the likelihood of referrals, and previous referral partners also no longer wanted to be associated with such providers for fear that the taint would wash off and affect their own relationships.
For this reason, making a very public name change to indicate new ownership was a smart move in order to disassociate from previous activities. However, the choice of Vertava Health as the new organization’s name was less than advantageous, and entailed SEO repercussions that the organization was not equipped to handle.
First of all, what does Vertava Health mean? While brand names can become associated with a product/service over time, this is a large lift from the marketing side of things. For Starbucks to become synonymous with convenient coffee or McDonald’s with fast food, there were massive, decades-long investments in marketing to make those household names. A smarter route is to have a name indicative of the product/service. In this sense, “Addiction Campuses” had been an intelligent choice. There is also a minor SEO benefit to having your service in your name (though not enough to make it a primary consideration of name choice, as some new providers fret about).
What does Vertava even mean? Nobody knew. It was actually the combination of two Latin words, meaning “right/truth” and “turn,” with the combined meaning of “right turn.” Which average American or referral partner was able to piece that together? Nobody. Was Vertava a physical therapy, home health, or pharmaceutical (the most common guess) company? Nobody knew.
Name Change Impacts on SEO
More importantly for the needs of the business, a name change entails a website migration to a new home. This means that the old site, which Google knows and recognizes, now becomes a completely new site under a new name. Google cross-references an organization’s name across the web as one way to validate rankings. All of the references Addiction Campuses had built over 4 years would not support Vertava Health as an entity on Google.
Additionally, migrations are serious business, especially for an organization reliant on SEO as one of only three marketing channels. At the time, Vertava Health’s marketing team was all internal. How often does an internal team migrate a website? They’d likely never done it. Very specific procedures need to be followed to migrate a site appropriately to ensure the least drop in rankings possible.
While vertavahealth.com no longer exists, so we can’t show the data using third-party tools, this information was publicly searchable with the right tools. If you had looked prior to the site going offline, you would have seen vertavahealth.com take a nosedive, losing 70% of its traffic 24 hours after the internal team initiated the migration in the summer of 2020. It was a total disaster. The organization had not been properly prepared for the migration and clearly didn’t have the internal talent to make it work.
It was at this point that Circle Social was brought in to fix the mess. Having to reverse and then redo the migration process resulted in an immediate improvement, gaining back 40% of the lost traffic (again, previously viewable with any third-party tools), but the damage had been done. Google does not like mismanaged migrations, and it takes time to regain “trust” with Google after such an incident. In short, the name change was a disaster, one that Vertava Health never truly recovered from.
A Name, Just Like Any Other
Despite these massive challenges, if the organization had invested in building a name for itself, it may have been able to surmount these difficulties in the long run. However, this never materialized.
Using the Way Back Machine, we can still view the old vertavahealth.com site. If we compare it to any other addiction treatment provider site on the web, can we identify anything that stands out? We find the same solutions and language offered on every other provider site. Treatments are “evidence-based”, “tailored”, supporting “addiction and co-occurring mental health issues.” This is the same thing found on most other provider sites across the web, even today.
Remember, Vertava facilities were located 2 hours away from major metropolitan areas where similar competitors were stationed. If a patient, family, or community referral partner is comparing two providers, which are largely indistinguishable from each other, will they choose the closer one or the farther one? Most of the time, they choose the closer one.
Admittedly, differentiation is quite hard in the behavioral health space. Unlike broader healthcare, outcomes tracking is few and far between. Ask any clinical director or individual therapist what best practices in care delivery are, and you’re bound to get as many different answers as the number of professionals you ask. That’s a challenge the field is still struggling with.
Yet, with that said, the most successful treatment providers in the country are the ones that have found ways to set themselves apart. This can be through care delivery, focus on specific disorders or demographics, admission logistics, community partnerships, and many more. Trying to fill 100-200 beds a month without clear differentiation, compelling patients to make the journey to an out-of-the-way treatment program is always going to be a losing proposition.
The right move would have been to truly dig down into the organization’s capabilities, then build a differentiated model setting itself apart from competitors. From there, heavy investment in marketing campaigns trumpeting the updated model, campaigns not concentrated in Google Ads, SEO, or the outdated tradition of horsetrading. Those three marketing channels are for people who don’t know where to go.
Those who go to McDonald’s for fast food didn’t do a Google search online for “fast food near me” because they already know where they want to go. Those searching for “addiction treatment near me” are on Google because they don’t know where to go. While this provides an opportunity for a provider to get in front of these searchers and potentially get their business, it’s also an indication of a failure by providers to build up a presence or reputation, one that Vertava Health could have filled with the right strategy.
We should note here, however, that such massive strategic shifts are very difficult for an organization already in free fall. As the late Clayton Christensen points out in his book, The Innovator’s Solution, organizations under capital constraints or in the middle of any kind of turnaround often struggle to break free of old tactics to invest in new ones. In this sense, Vertava Health was no different from Elements Behavioral, Solid Landings, Sovereign Health, Delphi Behavioral, American Addiction Centers, and all the others that found themselves in similar positions, each failing to pivot to avoid bankruptcy.
When “what got you here, won’t get you there”, it’s very hard to figure out what next steps are because the previous data, tactics, and strategies no longer provide insight for future success, especially if all other comparable organizations have failed as well, offering no alternative models or pathways. That’s a tough place to be for an executive team.
The HoldCo Model: Tales of Random Growth
Marketing and brand name changes were not the only missteps made by Summit Partners. With Vertava, they also engaged in a series of non-synergistic de novos or acquisitions. Before selling off the residential facilities in 2023 and 2024, Vertava purchased an MAT provider in Tennessee, opened a handful of IOPs in Ohio, and acquired an outpatient teen treatment provider, Connections Wellness, in Texas.
None of these acquisitions were synergistic. While we are strong advocates of a hub and spoke model for residentials and IOPs, the IOPs built by Vertava were in smaller suburbs. The purpose of a hub and spoke model is for the residential to fill the IOP and vice versa. Providers must look at their admissions data, determine where most of their residential patients come from, and then build IOPs in those cities. Instead of building IOPs in Cincinnati, Cleveland, Columbus, or Dayton, Ohio’s biggest cities, where, invariably, most patients would come from, Vertava opened up programs in small suburban cities.
This meant that the IOPs were, for all intents and purposes, separate businesses that needed to fill themselves with residents of those suburbs. Because IOP is 3 hours a day, 3 nights a week, most people will only attend an IOP in their city of residence. While there could potentially have been synergy with the IOP eventually referring inquiries needing higher levels of care into the residentials, that’s a large marketing lift to establish a new presence. Additionally, suburbs have much smaller populations than large cities, so they were comparatively limited from a total inquiry volume standpoint.
Not surprisingly, Vertava shuttered or sold off the de novos shortly after opening them. Its other acquisitions were equally non-integrative. Vertava had no facility presence in Tennessee, so the acquisition of an MAT provider, which often serves only a 10-mile radius around the facility, did not provide reciprocal referrals between programs/locations.
Connections Wellness was a teen outpatient provider in Dallas. Teen programs rarely get calls for adults, and vice versa. While there may be the occasional referral, these programs are, again, not synergistic. Teen treatment is an entirely separate business model requiring different marketing, different program delivery methods, different staffing and licensing, etc.
This HoldCo model of buying up random acquisitions that do not complement each other is, for whatever reason, SOP in the behavioral health space. If we look across various PE entries into behavioral health, we see this playbook implemented time and again. The thesis seems to be that “more” or “bigger” is better by default.
We strongly disagree and see no evidence of this being the case unless there are clear advantages. For example, offering all levels of care and taking all insurances in a given market, like Dallas, means that an organization can maximize its return on marketing spend. Rather than referring out inquiries for a level of care they don’t have, effectively eating that marketing spend, they are able to admit the patient into their own programming.
The same would go for a provider that had both adult and teen programming at the same level of care. Community residents and referral partners would eventually come to know that, regardless of age, they only need to call one provider.
While Vertava’s acquisitions may have been profitable as stand-alone entities, there were no synergies between the acquisitions. Vertava was merely acting as a holding company, which doesn’t provide overall value creation from our perspective. Would a strategic buyer or larger firm be interested in the individual entities? For example, would a provider with a network of adult outpatient programs in Dallas potentially be interested in acquiring the teen treatment programs? Definitely. But they certainly wouldn’t be interested in the random MAT provider in Tennessee or the residentials outside of Texas. In the same vein, the now disparate entities under the HoldCo were not attractive to outside investors, which is why the residentials were sold off piecemeal.
Misaligned Value Creation
Summit Partners has no public information related to its investment thesis, but we can reasonably reconstruct it based on the actions they took through the acquisition, holding period, and eventual sale of all Vertava Health facilities. We also don’t know if Summit Partners made or lost money on the deal. They sold off all the Vertava Health facilities and were perhaps able to sell for a profit or at least break even. Details of these deals were not disclosed.
But, with the rapid divestiture and complete exit from the residential treatment space, we can be confident that they found their original thesis lacking. Reviewing all of the above, where was the disconnect between the pre-acquisition thesis and actual outcomes?
No Field of Dreams
Speaking from viewing dozens of investor and PE-backed pitch decks in SUD, almost every one has a slide on the “unmet demand” for behavioral health treatment. We can assume Summit Partners was no different.
The thinking went that all one needed to do was acquire locations, and programs would simply fill themselves due to all the demand. This hasn’t been the case since at least 2015, when the number of providers across the country exploded. Marketing expenses at the time of acquisition, and still today, are significant.
Undifferentiated Value Prop to All Stakeholders
Because the Field of Dreams thesis was central to value creation, nobody paid attention to the operations or care model. Vertava continued with the same generic offering that Addiction Campuses had been providing. Addiction Campuses “success” was largely in their massive marketing spend, dominating search results at a time when destination treatment was still viable and there was enough crisis inquiry volume to sustain 100-200 bed facilities regionally.
With a national or even regional market domination strategy on Google no longer viable, Summit/Vertava failed to pivot to meet the needs of the new emerging market dynamics. They continued to offer the same treatment model that their competitors, who were much closer to most potential patients geographically, did.
With the previous foundation crumbling, no new foundation was being built to replace it. Instead, time, money, and effort were spent trying to patch up ever-expanding cracks.
No Economies of Scale
A standard PE playbook in healthcare is the Service Organization model. We see it with dental clinics, veterinary clinics, hospital ERs, and others. These are simple, highly successful models. Service organizations achieve economies of scale with costs spread out over multiple locations by aggregating backend operations such as marketing, billing, and staffing.
This doesn’t work in behavioral health because expenses scale with size and number of locations. Serving more patients? You now need more billing, more marketing, and more staff. There is no cost savings. Even leadership doesn’t scale. Because these are service-intensive businesses, adding on locations eventually means adding on levels of management at the local, regional, and national levels.
DSOs, in particular, are quite easy to scale because most dentists are owner-operators. They are heavily involved with the business and want to see it succeed. ER docs have significant financial incentives keeping them in one place. Direct care providers in behavioral health are rarely owner-operators and do not have the financial incentives to prevent high turnover. They have no skin in the game. Even facility leadership tends to be transitory and requires constant oversight or direction. This high level of hands-on involvement is not conducive to a service organization model.
Adding Locations and Service Lines Without Integration
Besides contributing to aggregate P&L, the HoldCo model implemented by Vertava provides no additional value creation between holdings. One could buy a series of residential treatment programs, a car dealership, and a CPG brand.
For a HoldCo model to function as an engine of value creation, synergies must exist between acquisitions regarding service lines, locations, and demographics served. Without that, each acquisition is just one more disparate business to manage, adding complexity to an already difficult-to-manage model.
What Insights Does This Provide Us Today?
As we can see, business drivers and models have changed drastically in SUD in under five years. Many of the dynamics that led to the failure of the Vertava Health thesis are still in force today. Successful programs are:
- In-network
- Local
- Offer a full continuum
- Have higher patient volumes utilizing lower levels of care
- Implement reputation-focused marketing
- Provide a differentiated service
Vertava Health, as a case study, provides a useful framework of what doesn’t work today to help avoid similar missteps and is instructive regarding more efficacious models.
Looking for help with market entry, growth, or turnarounds in healthcare? Get in touch.