
I’ve been coming back to the question of how to build a national program a lot lately. I hear it from providers big and small, investors, and even REITs in this space. Many organizations have experience, there’s a ton of capital floating around for behavioral health investments these days, and yet everyone that has gotten large enough to pay attention to has either failed or is finding growth to be a much slower process than they originally thought.
Many have tried: AAC, Sovereign, Elements, Foundations, Delphi, Vertava Health, JourneyPure. Others are trying now. But no one seems to have found a way to quickly build a nationally recognized behavioral health or addiction treatment program. Even Hazelden, a program that’s been around for 50 years and is one of the best known in the nation can’t grow beyond its current size. Why is that?
There are no definitive answers, but we’ve been able to identify the most common challenges. If different types of providers could learn from each other’s strengths, they’d have a strong opportunity. We’ll look at this in 3 sections: Old Guard Non-profits, The New Vanguard of For-profits, and Current PE at Scale
The Old Guard Non-profits Aren’t Built for Scale
There are many programs that have been around for decades. Some have added a level of care or two, maybe they started to take in-network insurance and added some beds, but most of these programs haven’t grown much, Hazelden in 16 locations across the country being the only true exception.
Even though many had first mover advantages, most are still a single facility. There are several factors as to why that’s the case:
Cater to a high socioeconomic demographic.
Most of these programs started when cash pay was the name of the game, meaning that only the very wealthy 1%, at best the top 5%, of the population could afford treatment. Older programs still mainly cater to that demographic and it’s, by definition, a small population. It’s not possible to scale a program across the country that the vast majority of Americans can’t afford.
Related to the demographic often served are extremely high labor costs.
Because programs catering to the wealthy require a higher level of clinical care, they don’t have a model that is cost-effective if they were to rely only on in-network reimbursement rates. These programs often don’t want to compromise the current quality of care they deliver by hiring less staff or less-experienced staff. This is great for patients in these models, but does significantly limit growth opportunities.
Compensation for non-clinical staff is often substantial at higher end programs; they’re often renowned in the field or come with Ivy League degrees. Additionally, some of the highest-paid Business Development and Call Center Admissions teams come from these programs as well. As many of the for-profit programs will tell you, paying six-figure salaries for Call Center Admissions or Business Development staff is not scalable with in-network reimbursements. Normalized salaries mean more turnover and a stronger reliance on systems and processes over key staff. More turnover and the hiring of less experienced staff means that more inquiry volume is needed because staff are converting a lower percentage of inquiries to admissions.
Older programs’ staffing models won’t work at scale when expanding into other patient demographics.
Reliance on alumni and well-established referral relationships without effective build up of other marketing channels.
For older programs, it’s often the case that 50% or more of their admissions come from alumni and alumni referrals. For example, I was talking to an alumnus of an older program. He went through the program, then his brother, then his dad, then his dad’s brother, then his friend. He also re-admitted once and I didn’t ask, but statistically speaking at least one of those other referrals did as well. So one admit turned into seven. That right there is the business value of having an excellent program, very high referral volume. It’s something newer programs could definitely learn from, which I’ll discuss later on.
In the world of Silicon Valley or trendy business magazines, this would be akin to “building a community of raving fans.” The difference is that, unlike products that appeal to the masses, alumni referrals alone aren’t very scalable. Again, most of these programs are focused on a very small, wealthy segment of the population and they only have a limited amount of referrals to make in any given year.
The referral network of the program and the Business Development team is similar. There are usually limited systems in place to find new referral partners. Instead, there is a strong reliance on decades-old relationships, and many of these long-term referral partners have reached retirement age. Older programs also used to refer to each other a lot since programs had different levels of care and accepted different insurances. That dynamic has changed with more programs building out full continuums and accepting a wider range of insurance.
Neither long-established referral networks nor alumni referrals are scalable to a new facility. If you try to take a Connecticut-based program and open another facility in LA, those admissions streams won’t follow to the new location.
To be scalable, a program needs systems and processes that can be established in new markets and can be relied upon for growth without a pre-existing base.
If you look on the backend of most well-established programs, you’ll generally see that the majority of their search volume comes from brand searches. This means that people who are already familiar with the program, have done their research, and have already decided the program would be a good fit, are the ones finding the website and calling. It’s quite easy for a call team to convert inquiries where the caller has almost made up their mind before calling.
On the flip side, programs like the AACs, Sovereigns, and Elements of the treatment world were able to scale and grow so fast at one time in the past because they had repeatable systems for attracting patients in newly established markets without reliance on previously well-established ones. It turned out that the methods they were using were too expensive to be sustainable after reimbursement rates got cut, but they were on the right track in terms of the need to figure out that process.
Ethical, patient-centered marketing does work in new markets, it’s just a lot harder because you have to be really good at it to deliver cost-per-admissions that work with in-network rates and it requires more time. The model that failed was driving massive amounts of inquiries and only converting at 1-3% while also artificially inflating conversions by paying for flight costs. That pray and spray with massive marketing and call center investments only worked when the reimbursement rate covered all the excess, which is why you can still find a couple small OON providers here and there grasping onto a dead model.
The newer for-profit programs, when they first started, also gave a bad name to rehab marketing in particular. For this reason, there is a lingering distaste among older providers for online marketing.

This is unfortunate as this mindset holds these programs back. Marketing on any channel where patients are, and online is the place to find a lot of people who need help, is critical to fulfilling one’s mission of connecting people to care. If patients don’t know your program exists or why they should choose it over calling the shady lead aggregator number they just found in a Google search, then you’re not only failing them, but also limiting your own program’s growth. Good marketing is value-added and mission-driven. Even better, good marketing drives better results than the shady tactics of old, which is why none of those models worked in the end.
When I first started Circle Social, it took quite a bit of convincing to get people to believe that mission-driven marketing would not only get results, but deliver them at a lower cost than anything they’d seen before. More than 100 facilities, 26 full-time staff, less than 5% client turnover per year, and industry-leading CPAs has proven us right time and again.
Narrow recovery model
Most older programs have a very narrow recovery model, almost always 12-step. As we all know, 12-step works extremely well for some people. However, as the older providers in the industry have only slowly begun to accept, other recovery models work much better for different people. To effectively scale, one needs a clinical model that can help as many people as possible. A one-size-fits-all approach restricts potential patient volume needed for growth. This is especially true as Christians become a smaller and smaller demographic in the US, at 65% down from 85% twenty years ago. Protestations to the contrary that 12-step is not only for Christians aside, 45% of patients across the country do not want faith-based programming, which is why growing programs have moved away from only offering Twelve Step Facilitation as a modality.
Lack of desire.
Finally, the OON and private pay model is very lucrative with high margins. Owners and staff are compensated far above levels seen at for-profit businesses of comparable size.
These programs are also committed to providing the higher level of care that the high margin model affords them, so they don’t have to compromise quality to serve more patients in order to maintain financial solvency and then some. As mentioned previously, this is great for patients, but puts challenges on the model in terms of potential patient pools.
I had a conversation with the executive team of one of these higher end programs a couple years ago. I told them they would not be able to survive at their current size on OON only and would eventually have to go in-network. They responded that lowering the quality of care to operate on in-network reimbursement rates was not something they were willing to compromise on. While they did hold out for a while, this year, they just moved in-network with a number of payers. As others have found, you have to stay relatively small if you want to survive on OON or private pay patients only.
PE isn’t involved in this world, so there is no engine creating urgency around growth in value. With few exceptions, the mission is to drive quality care within the existing program rather than expand care to a wider range of people. Many of these programs know who they are and know who they want to serve, so they are content to maintain their current size.
Lessons Learned
-
Focus on quality programming differentiators drives long-term reputation that lowers marketing costs.
-
Cultivating alumni and healthcare professional referral relationships pays long-term dividends (and improves clinical outcomes by keeping alumni connected to a support network).
-
Narrow focus in terms of both recovery model and demographics served limits growth potential.
-
High-touch models have high labor costs that also limit expansion potential.
-
These programs do an excellent job of creating a “community of raving fans,” but a poor job of creating repeatable systems and processes for high volume patient inquiries in new markets.
New Vanguard Is Stuck with Legacy Models
I see the greatest challenge for new programs, often for-profit, is that they are stuck with facilities, systems, and staff that were ideal for an older model that no longer works in the current consumer and reimbursement environment. Let’s take a look at the different challenges:
Facility locations
Healthcare is local. It always has been. The misconception in behavioral health that it was a destination arose from high-end programs that cater to the wealthy. For most of our residential clients, 70% of their admissions come from a 70-mile radius with another 25% coming from a 150-mile radius. PHP and IOP with housing are the same, without housing is 30 miles. Psych hospitals and MAT clinics are also 30 miles. As we’ve discussed, relying on fly-ins or asking patients to travel greater distances because the facility is far away from urban areas is a very difficult model to scale.
The temporary oversight on the payer end for sky-high reimbursements and the lack of regulation in the industry created a moment in time when patients could be flown to inpatient programs, but we all know that’s no longer the case.
This has left some larger providers with very expensive properties far from urban areas where most of the patients who need help are. A program 30 minutes from LA is a lot easier to fill than a program 2 hours away from it.
Nowadays, it also affects a website’s ability to rank in Google search. Google has deliberately tweaked their algorithm over the years to prioritize local rankings for behavioral health searches. Local ranking requires a verified Google My Business tied to a legitimate business in the city. From a Google ranking perspective, a program in LA will always have significant advantages over a program just outside the city. Have a program in the resort town of Lake Arrowhead? You’re going to have to spend four times as much to show up high in the search engine results in LA.
Another legacy challenge related to location is that larger providers often have locations in many different states. Logistically, this will always be harder to manage compared to geographically concentrated facilities and can contribute to higher than manageable HQ costs.
High HQ costs
Older reimbursement environments enabled extremely high HQ costs – call centers with 50+ reps making six figures or more, exorbitant nationwide marketing spends of a million dollars a month or more, nationally dispersed Business Development teams with more six-figure salaries managed primarily from HQ, and generally bloated staffing. This centralization also created a lack of accountability or authority for management at the facility level in terms of P&L. When census is down, responsibility falls solely to HQ rather than local Directors. Centralizing departments such as billing, marketing, HR, and operations has a number of advantages, but must be done in a way that HQ can be supported through current facility revenues. That’s easier said than done.
Staff recruitment and training
Executives get it now. Healthcare is local and referral partners need to come from a variety of sources in the community.
Who doesn’t get it? Many of the Business Development Teams out in the communities. In addiction treatment, they’re still too reliant on horse-trading around levels of care or different insurances. It’s not uncommon for me to hear a strong community-centric approach from the executive team, but then speak to one of their Business Development Reps at a conference who is doing none of it and relying on old habits.
I’ve been talking for the past couple years of how this is a dead-end form of marketing. Most providers have extended their continuums of care and many take most kinds of insurance, so there isn’t an opportunity to “trade referrals” at a level that is sustainable for census. It’s taken longer than I originally thought for a better model to take hold.
In many programs, I also find that reps don’t know enough about the program. They’re trying to get referrals, but are often focused on techniques like donut drops without truly understanding the nuances of the program they’re representing. This lack of knowledge makes it unlikely that they’ll be able to build referrals from the healthcare community. Add to that the pressure to get more referrals right now this instant, and we end up with a situation where reps simply go back to what they’ve done in the past rather than spend the time building out the skill sets and relationships needed to connect with other professional community partners.
As facilities hire more reps in efforts to grow admissions, they often end up with increased labor costs and not enough to show for it as the right relationships aren’t being built in their territories. Time passes, pressure builds, and reps resort to ineffective scrambling. This is why solid training and pre-built playbooks are needed to create an effective business development team.
Build reputation & differentiators
Whether we’re talking addiction treatment, psych behavioral, or MAT clinics, reputation is critical to success. We see this success mirrored in the older programs that have almost all of their admissions come from alumni or long-term referral partners.
In the for-profit space, there has been an overreliance on SEO, Google Ads, and Business Development Reps who are constantly on the move looking for a new referral. What newer programs can learn from the older programs is that a quality program that builds reputation over time significantly reduces marketing costs.
This is business 101. In the beginning, every business will struggle to convert new customers because there is no consumer mind-share or reputation already established. When we see the McDonald’s golden arches, we automatically know it means fast food for cheap. McDonald’s no longer has to spend advertising dollars or air time in their commercials to tell us that. The arches say it all and they can use their advertising dollars to focus on other messaging, like new products.
But that reduction in marketing spend and amplification of community mind-share can’t happen without investment in long-term advertising. If every patient finding a program is coming from a Google search or a BD rep just happening to come across a new referral partner at the right time, those costs will be incurred every month again and again. The patient didn’t admit because they wanted a specific facility, they just called because the Google Ad popped up at exactly the right time.
Shift that to when a provider is well known by residents of the community as well as professionals, now admissions will come in from people seeking out the provider with no need for a marketing spend PLUS admissions will continue to come in from the Google Ad showing up at just the right time.
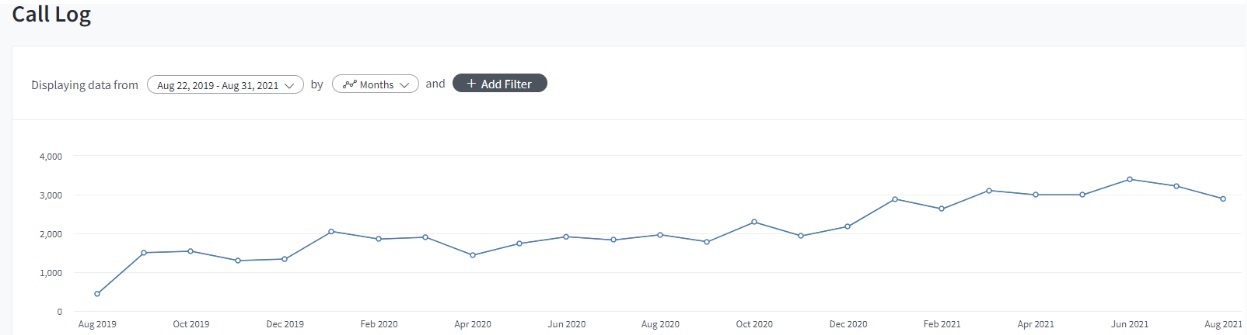
We see that clearly in our own data across clients. Here’s an example of one client where call volume doubled over the past two years we’ve been working with them without increasing marketing spend.
Below, is a screenshot detailing the number of days it took for a visitor from their first visit to the website to make a call. It’s from two years ago, before we started with the provider, and you can see that 90.5% of all calls came in the same day as the first website visit. When programs invest only in what I refer to as crisis-focused marketing, they only get patients through referral partners and Google search who are desperate for treatment now. But we estimate that that is only 20% of all commercially insured patient volume in a given geography.
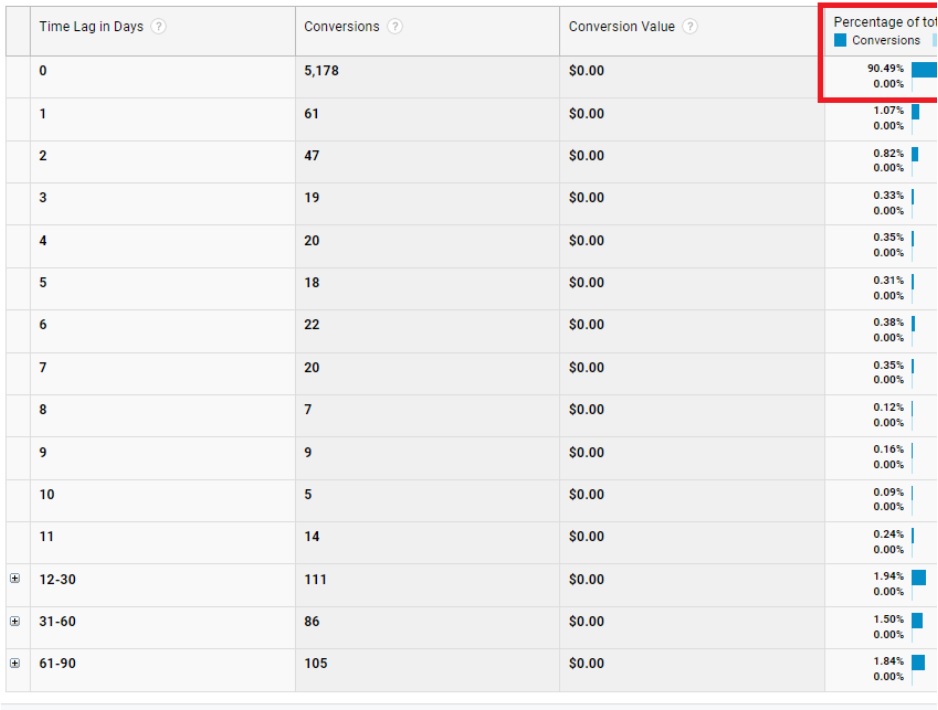
The other 80% are not coming from the ER or doing a Google search in a moment of crisis, they’re considering and contemplating when, where, and if they should go to treatment.
So in the above screenshot, you can see when we started with the client, they were reliant on crisis marketing through Google search and business development only. The people hitting their website found it at the right moment and called immediately 90% of the time.
Fast forward to two years later after we implemented long-tail marketing channels and you can see from the call log screenshot above that their call volume climbed to double what it had been on the same marketing spend. This is because the long-tail channels, such as Facebook, OTT, TV, and radio create cumulative inquiries and admissions as mindshare is built up in the community over time.
The Google search or ER volume on any given day is fixed. There are only so many people in crisis on any given day. The vast majority who need help are not in crisis at this moment, but when you reach out to them through these other channels, more and more start to call as awareness and trust is built up.
This is why we see that, over the last eight months of this year for this same provider, only 63% are crisis calls coming in the same day. The other 37% are calls from people who have been visiting and researching the program for months, which is what we want to see.
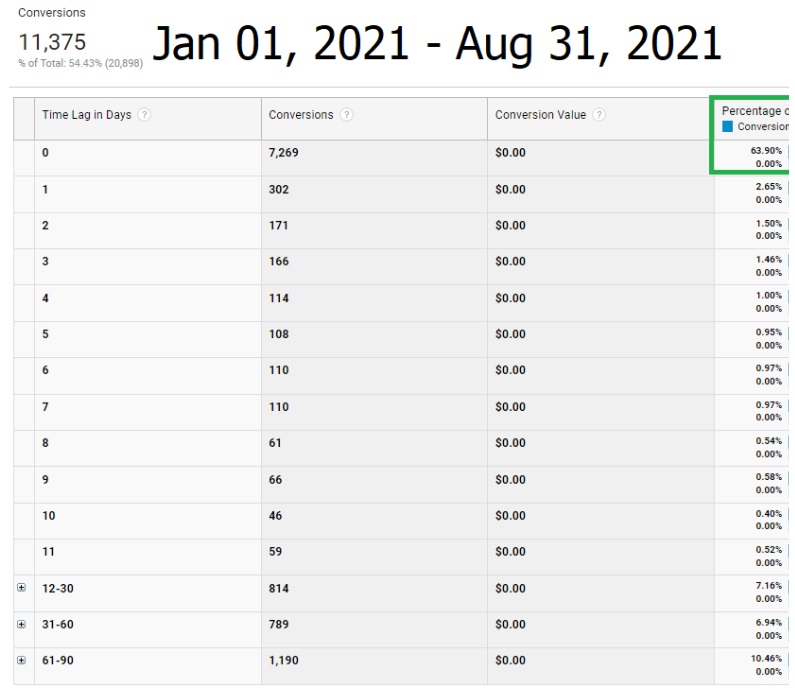
On average, half the visitors visit the site at least two times in separate sessions before calling as seen in Path Length interaction tracking below. As that percentage is higher than the same day call percentage, it tells us that 10% of those who call the same day they first visit leave the site and come back later to make the call.
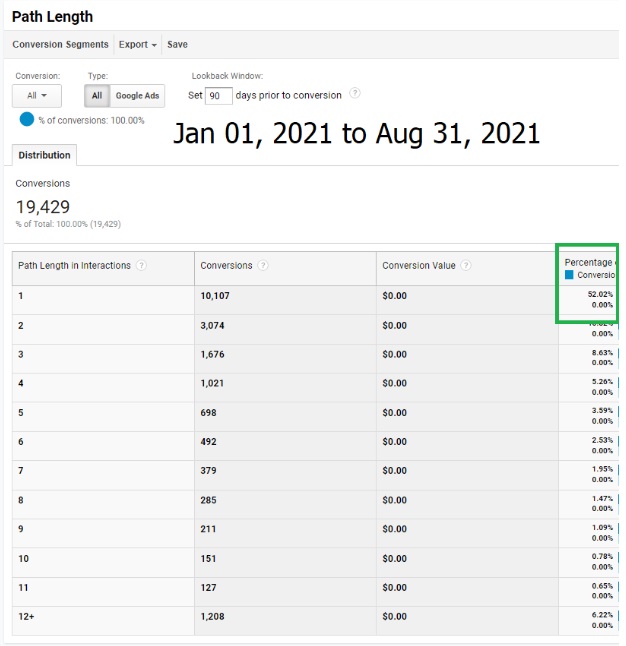
Our data shows that most people tend to call within a 1 to 3-month window from their first site visit.
Lessons Learned
- Build new programs near urban areas with high population density or understand the need to pay more for increased marketing to cover a broader area and build up a higher level of trust that encourages patients to travel farther distances.
- Programs need to train new hires or retrain existing Business Development Reps on clinical care and how to liaise with professionals in their communities outside of the treatment space.
- Investments in marketing spends outside of final attribution are needed to drive patient inquiry volume from non-crisis sources and reduce marketing costs long-term. Note that non-crisis calls require more highly skilled Call Center Admissions Reps as well since callers are researching and carefully evaluating programs, not just admitting into the first place they talk to that has a bed and takes their insurance.
- These programs do an excellent job of creating repeatable systems and processes for high volume patient inquiries in new markets, but a poor job of creating a “community of raving fans.”
Smaller Opportunity Than Originally Thought Limits IRR to Fuel Growth
I’ve spoken about this a lot, but there isn’t as much demand as once thought, meaning there isn’t the patient volume that was supposed in many a pro forma. Let’s take Indiana as an example.
It has a population of 6.7 million. Only 53.9% have commercial insurance, so 3.5 million. About 1.5% of the commercially insured use their policies for SUD/AUD. Now we’re down to 53,265. Of that, 15% will use a form of intensive treatment such as residential. That’s just under 8,000 people. Dividing that by 12 months of the year, Indiana can support roughly 660 residential beds for the commercially insured. At an average reimbursement of $15,000 per patient, that’d be $120 million in revenue per year. Certainly a decent amount of room there for a couple businesses, but much less than what’s proposed in most decks to investors.
There is the usual caveat that only 11% of people that can be diagnosed with an SUD/AUD seek treatment, which often leads to the supposition that there is a “blue ocean” of opportunity in reaching those who aren’t seeking care. However, as SAMHSA has pointed out in their studies, the other 89% have explicitly stated they do not want to seek formal treatment. So it’s not a matter of getting the message out to those who don’t know treatment exists; it’s a matter of educating and convincing those that are aware of treatment options, but don’t want to go. That’s a very difficult proposition that requires significant investment in marketing costs to change minds, so not a good business model if near-term growth is the goal.
Private Equity Hasn’t Built Platforms
Many of the early PE models that have existed to date have largely been simplistic stacking, what I refer to as a holding company model. They have one facility doing 20 million in revenue, then acquire a second facility doing 20 million in revenue. The only thing that has changed is that the two revenue streams are now under a single bigger company, but additional value has not been added in either business.
From our perspective, the real value of roll-ups is by creating additional value that did not previously exist. This can be through de novo builds or by creating platforms and economies of scale across acquisitions, such as:
- Can billing, marketing, or other business units be centralized to lower cost and increase expertise?
- Can skill transfer happen across facilities that improve new acquisitions in a way that increases revenue or lowers costs? This is a large opportunity in clinical. Testing pilot programs, tracking outcomes data, finding what works best, with a lot of programs and a lot of clinicians, there is great opportunity to define and disseminate best practices.
- Can uniform technologies be implemented to lower costs?
- Can a regional or national brand be established to reduce marketing costs long term?
Most PE initiatives in the behavioral health space have not done a great job of the above to date. In the addiction treatment space, there is some centralization in an HQ, but this was usually done prior to PE involvement.
The focus needs to be on creating additional value rather than the simple stacking of revenue streams.
Putting It All Together. What’s the Opportunity?
New providers can learn from older ones the value of investing in strong referral relationships, a reputation for differentiated clinical, and alumni programming, basically building a community of raving fans. Older programs can learn from newer ones how to branch out and create systems and processes that expand patient acquisition channels outside of the ones they’ve relied on for such a long time. They also need to rethink how they view marketing as it connects to their mission. Additionally, older programs could learn how to lower cost structure to accommodate more patients on in-network rates.
Any provider trying to scale can benefit from focused efforts on the local nature of healthcare, from facility site selection to Business Development Rep community integration to geographically tight marketing campaigns. Both older and newer programs can also benefit from investment in long-tail marketing channels that drive cumulative inquiry volume over time. Older programs have done an excellent job of creating a reputation and brand among referral partners and alumni, but have not learned how to do the same on traditional or digital marketing channels. Programs need to expand their capabilities in traditional and digital media outside of only search-intent, crisis-focused inquiries where volume is limited.
Creating a centralized HQ and repeatable processes that can be implemented both with de novo builds and acquisitions is also key. This goes beyond just billing and marketing, but expands into HR, especially recruitment, training, and retention. More importantly, leveraging data, best practices, and talent across the organization to create economies of scale that drive down costs as well as improve quality and reputation at the same time.
While there are areas of the country that still represent an opportunity where supply hasn’t met demand, I believe the greater opportunity is building a scalable program with a strong reputation that enables the provider to outperform the competition because, these days, competition is everywhere. In many markets across the country, we’re at the stage where census rising in one program comes at the expense of it falling at another. So expansion is less about finding areas of unmet demand and is more about becoming a leading provider. Leading providers that have the potential for scale should be able to answer these questions:
- Can you provide better care at lower cost?
- Have you worked to lower barriers to accessing treatment such as cost, travel, speed of intake, and insurances accepted?
- Do you have a cost-effective marketing engine for patient acquisition, this includes long-tail awareness, trust, and reputation builds so you’re not reliant only on crisis inquiries?
- Are clinical, business development, and marketing in alignment so that what’s communicated to patients and referral partners is what they get in the program, thereby building patient satisfaction and reputation?
- Are alumni and community healthcare professional communication strong and consistent in order to drive low-cost word of mouth and referral volume over time?
- Are KPIs and outcome metrics in place to enable identification of areas for improvement across business units?
- How do you keep HQ costs at a reasonable level while taking advantage of the cost savings brought about by centralization and also still providing facility-level directors with levers they can pull to improve their own P&L?
- Do you provide a differentiated level of care that is hard to find or difficult to deliver? Does your program offer something competitors find hard to copy successfully to prevent competition while increasing patient/referral partner preference for your program?
- Are your systems and processes repeatable and scalable to enable consistent implementation upon expansion?
- Are you able to recruit and retain staff while training them on the unique aspects of your care delivery?
If you can come up with answers to the above and, as always, consistently execute, then maybe your program can be the first to crack the code and create a nationally recognized program across the US with the ability to grow quickly.
If that’s your goal, or you just want to be the preferred provider in your area and need help achieving that, get in touch with us at circlesocialinc.com or call 800 396 9927.