
Private equity, especially lower and mid-market firms, continue to seek investments in the behavioral health space (SUD and mental health). However, instead of achieving returns, many end up with sizable write-downs and losses. There are very clear reasons for why this is. Having worked with numerous private equity firms, strategic buyers, and investment groups, we see the same mistakes made again and again. If you’re planning to invest in the behavioral health space, or have already and are struggling, this article will outline the most common mistakes to help you avoid them or course correct.
Where Are All the Patients? Re-Evaluating the Thesis
First and foremost is that firms enter the behavioral health space with the wrong thesis. For 10 years now, we’ve seen the same slide in every pitch deck, “Only X small percentage of people that need care, receive it.” The thesis is then that there exists significant opportunity to further provide services to those struggling with substance use and mental health issues. Following from this is the idea that marketing and community outreach is cheap and easy. All one needs to do is open up and the patients will basically flood in.
This thesis is dead wrong. While it is true that most of those struggling with a diagnosable disorder do not enter treatment, it is false that they want to enter treatment, especially at higher levels of care. According to SAMHSA, only around 11% of patients with a diagnosable disorder actually want to receive care in any given year.
This means that the total addressable market is much, much smaller than the pitch decks would lead one to believe. The bottom line is that the market is already oversaturated with providers. There are too many beds for too few patients.
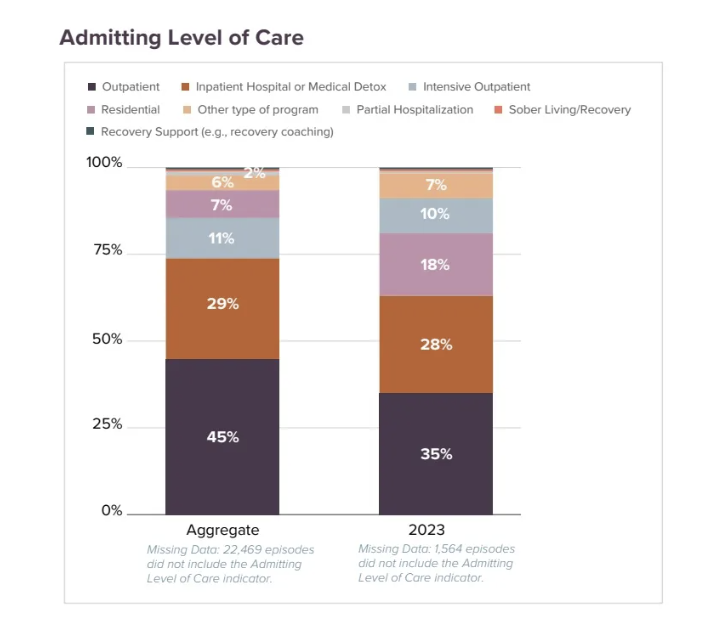
Here is some relevant additional data from the National Association of Addiction Treatment Providers FoRSE data tracking 130,000 patient episodes from 2018-2023 from providers across the country. As you can see, the majority of patients do detox and weekly outpatient programming. Residential, PHP, and IOP are the least commonly utilized levels of care, which just happen to be the levels of care private equity most commonly invests in.
Scrambling for More Patients
The firm comes in and buys a provider. Upon doing so, they quickly start to realize that patient acquisition seems more challenging than originally thought. At this stage, there isn’t much concern. The idea is that they simply have to hire the right marketing team or vendor who will solve the census problem quickly. This most often starts with a known vendor they’ve worked with before.
The known vendor is brought in and they are not able to fill the census. You wouldn’t hire a cardiologist to do a hip surgery, so why firms hire marketers without specialized experience in behavioral health, we still don’t understand. Legal complexity, highly tailored messaging requirements, platform restrictions for healthcare advertising, difficult marketing funnels, no run-of-the-mill agency will know any of that. Lots of money is spent with little result.
Back to the drawing board. The next step is to hire an agency that specializes in the behavioral health field. They interview several vendors with the main focus being on filling beds fast. For this, they expect to resolve the problem reasonably quickly using Google Ads, some SEO, and maybe some business development outreach.
Most of the agencies promise them spectacular results in record time. One, maybe two agencies, like Circle Social, don’t paint such a rosy picture. They tell them the reality of the high cost CPAs for Google Ads, diminishing returns, and the multichannel strategies with longer timelines that are needed to succeed in behavioral health.
The firm opts for one of the agencies promising spectacular results in record time. 3 months in, none of the touted promises made by the agency hold up. Census is still low and the patients that did come in off the PPC campaigns have such high CPAs that they’re losing money on every patient.
The firm is convinced it’s a numbers game. If they can just get the spreadsheet math to work, it’ll be fine. All they need is a lower CPA. They fire the first agency and hire one of the other agencies that had promised spectacular results in record time. Another 3 months goes by and, still, nothing changes.
With this saga ongoing, the same is happening on the business development (BD) side. Based on their research, the firm believes that a BD rep can bring in X number of admissions each month. Running the math, they determine how many BD reps they need to hire, then get them onboard.
But spreadsheet math doesn’t translate to reality. They quickly learn that BD hires are just as likely to overpromise and underdeliver as the marketing agencies they’ve been bringing on. Patient acquisition isn’t math. There are core competencies needed to successfully execute. For BD alone the org needs to know:
what good BD looks like and how to identify the best hires
how to train reps to be effective
what supporting collateral and marketing campaigns are needed to support reps
how to effectively deliver on the promises they’re telling their BD team to make in the community
what systems and processes are needed to most effectively facilitate relationship building and referrals
All of the above are necessary for a BD rep to bring in admissions. Like any business, success is in the execution, not in the identification of tactics.
All of behavioral health marketing is like this. It’s a reputation build that takes very knowledgeable investment in multiple channels to eventually drive success.
Healthcare Requires Time, Lots of It
Most investors tend to operate on shorter time horizons. It’s normal for investors to want to start seeing returns within the first year and for PE firms to exit within 5-7 years. However, behavioral health rarely operates on such contracted timelines. This is because healthcare is local and success is largely driven not by the most optimized PPC or SEO campaigns, but by community reputation. Reputation building takes a lot of time AND it requires excellence in execution. One can’t build a reputation in healthcare only through marketing. Instead, reputations are built through relationships and maintaining care delivery standards. The best marketing in the world won’t help a healthcare provider be successful if the care they deliver doesn’t meet the expectations of patients or community partners.
More importantly today, because there is an oversaturation in the market, it’s not about just meeting basic expectations. New providers or entrants must exceed expectations in order to beat out the competition. This is very important.
Expansion strategies require years of time to see return in behavioral health. While a provider may be very successful in its home market, this success will not translate to new markets because healthcare reputations are hyperlocal. Many firms will make the mistake here that they can simply open up de novo locations or acquire other providers to expand rapidly. Due to the reputation building requirements, this takes a lot of time, usually far longer than the firm was expecting or willing to wait. They try to rush it by rapidly expanding BD or scaling up the PPC spend. Firms end up in the same predicament with their new facilities as they have with the first one, low census and high overhead.
As an example of what not to do, a fairly large provider on the East Coast recently opened up a new location in Denver, CO. Why in the world would they think that’s a good idea, we don’t know. Denver is very oversaturated with providers, and high quality providers at that. Providers in Denver are fighting tooth and nail for patients as it is. Deciding to enter that market is a perfect example of a new PE sponsor pushing for growth with no real understanding of the market or growth potential. Instead, they’re expanding just to expand, which will come at a large cost and very little gain.
Buying and Expanding Without the Right Strategy
Firms often base their expansion strategy on the reimbursement environment or by finding an acquisition at a good price. This is why so many providers with PE backing end up sprawled across the country. As firms quickly find out, this is a recipe for disaster. The logistical complexity of operating across state lines with the different licensing requirements and payer landscape is not easy to overcome.
This is in addition to the fact that the new location has zero reputation in its new community of operation. As we’ve stated, local reputation is everything in behavioral health, so starting from scratch here is often the single largest hurdle to overcome.
The right way to expand is through a hub and spoke model. Expansion should occur in a circle around current operations, going just far enough out that one doesn’t cannibalize existing locations while also being close enough that the existing location’s reputation may carry over.
Our most successful clients are not successful because we have a brilliant PPC or SEO strategy. While our best-in-class results certainly don’t hurt, that marketing work alone is not enough to be successful. Focus cannot be simply on bottom-of-funnel spreadsheet math for the front door. They are successful because they:
Haven’t overextended themselves
Minimize logistical complexity by staying in environments they know
Expand outward in a way that enables them to build upon the reputation they’ve built in an area close enough geographically for that reputation to at least somewhat exist in the new location.
Continually build relationships among community referral partners, government agencies, and local healthcare systems.
Invest in diverse, multichannel marketing that includes both top-of-funnel and bottom-of-funnel strategies with appropriate expectations on time for return
Offer something that stands out in the markets in which they operate
The Core Differentiator in Successful Expansion Is Go-to-Market Execution
There is little economy of scale in behavioral health. Expansion requires more staff, more marketing, more billing, etc. So size does not bring much of an advantage in most situations. There are some advantages in payer contracting once a provider is large enough, but this is only a factor if the provider expands in the same state since different states have different payer entities and contracting environments.
Many providers struggle with expansion because they do not have repeatable systems and processes for expansion. In order to successfully expand, the organization must have expertise in the following areas:
Site Selection: This is not just reimbursement, this is identifying the right location for visibility and access, mapping out community referral partners, analysis of patient trends, and competitor analysis
Real Estate: Lease or purchase negotiation
Construction Team: If the site needs to be repurposed or remodeled, this team needs to know how to scale operations
Marketing: So many providers go in with no marketing strategy. They think they can plop down what they’re doing at current locations, but a new market strategy has very different requirements from existing locations, as we’ve discussed. Marketing budgets need to be double for at least the first 6 months and certain channels, such as SEO and BD, need to start months before a new location opens
Recruitment and Staffing: Long-term staff are an important part of provider success. The local talent pool is critical. If the new site is in a rural area or far out of town, finding qualified staff will be incredibly difficult
Licensing and Accreditation
Payer Contracting
Differentiated Clinical: Observe your clinicians lead a group or individual therapy session. Then do the same at a competitor. Does it look exactly the same? That’s a problem. Care must be delivered in some way that is different from other marketplace options, otherwise, why would anyone choose your program over the competition? Clinicians need to be trained on your program’s specific methods of care delivery. If you don’t understand What Good Looks Like in terms of clinical delivery, you better find someone who does and who can explain it to you. Clinical delivery is the core of the business, if you don’t get it right, you’ll fail and, if you don’t understand it, you should probably invest in something else that you do understand.
We’ll also add here again that new locations need to bring value to the market that they’re in. Far too often, providers expand with the same exact offering as multiple competitors in the same market. This is about as helpful as putting a Gloria Jean’s Coffee next to a Starbucks. Now two providers are competing for the same fixed patient base. This could potentially work if there were more coffee drinkers than the Starbucks location was able to service, but that situation is definitely not the case in behavioral health. Most providers have ample room, so there is no overflow to another provider.
In order to succeed, a provider must identify what value it brings to the market that other existing providers are not currently offering. Think like a Burger King moving next to a McDonald’s. While both sell hamburgers, the food offerings are distinct enough that consumers will prefer one over the other. Behavioral health providers need to operate in the same way.
If a provider can’t identify what they do differently or better than existing competitors in the new market, then opening there is going to be a mistake. As we’ve repeatedly mentioned, behavioral health is mostly about reputation. The existing competitors have established relationships and reputations. When your new BD rep goes to the hospital that has been referring to an established competitor for years, why would the hospital suddenly switch over or send any referrals to the new provider in town? They won’t unless there is something very unique and valuable about the care delivered by the provider which is not currently offered by their current partners.
Copying the Wrong Examples
During the height of the covid pandemic, TalkSpace, Cerebral, and BetterHelp all had sky high valuations. Every one of our clients big and small looked at them and said, “Wow, we could build a billion dollar telehealth company!” They all tried and failed.
Notably, the telehealth companies with the sky high valuations also ended up failing. BetterHelp is the only one still around of note. As part of Teladoc, it still hasn’t made any money here in 2024.
This trend is common in behavioral health. 7 years ago, the companies to model were Elements Behavioral, Sovereign, and American Addiction Centers, all of which subsequently went bankrupt.
The latest has been the $1 billion sale of Newport Health in teen treatment. It remains to be seen whether or not that purchase price accurately reflects the company’s underlying financials. If the history of deals in behavioral health is anything to go by, that is unlikely.
This has been a great challenge for providers and investors. They look to the biggest companies in the space assuming that their models are financially sound, so they begin to emulate their tactics. When they don’t work, they assume they’re doing something wrong, that there is still some secret they’re missing, when, in reality, the tactics they are copying have not been successful.
Spreadsheets and Short-term Metrics
A lot of investment firms are good at numbers and projections, but numbers don’t mean much unless the organization can successfully execute on its services.
One of our favorite stories is about a large PE firm that we were working with who had recently purchased one of the country’s largest providers after previous owners had failed. Upon acquisition, marketing CPAs were higher than projected. In an executive summary meeting, the Chief Marketing Officer pointed out that one reason for the high CPAs was the poor online review scores.
We know from our internal data that aggregate review scores under 4 stars increase CPA costs by up to 20%. Just like no one goes to a 3-star restaurant, patients don’t go to providers with low star ratings if there are more highly rated options nearby.
Later on in the meeting one of the PE Firm representatives introduced some calculations he’d made on his iPad. He stated that, in order to increase their review score from 3.5 to 4.2, all they needed was 34 more 5-star reviews.
So simple!
This story highlights the nonsense of a spreadsheet mentality. The math is easy, but actually delivering care so great that 34 patients want to leave a 5-star review is no easy feat.
Marketing and call center messaging must match patient experience. If patients get something different than what they expected, they won’t leave a good review.
Clinical delivery has to be positive and effective.
The patient’s experience with all other non-clinical staff needs to be positive.
Finally, there needs to be an effective process for soliciting such reviews. Most people don’t leave reviews, much less 5-star ones. Maybe only 10% of patients are willing to leave a review because who in behavioral health wants their name on the internet showing they went to a treatment facility? So, to get 34 five star reviews, a provider needs to deliver treatment to 340 individuals.
Again, the math is easy, but actually obtaining 5-star reviews is not.
An overemphasis on short-term metrics also has a very negative impact on organizational strategy. In most marketing meetings we’re a part of, 90%, oftentimes even 100%, of the meeting is focused on PPC because this is where a large portion of spend is going. This is a mistake.
Provider success is driven by local reputation, not by crisis callers off of PPC campaigns. This means that the core drivers of the business are community outreach, alumni, and outbound paid media campaigns across channels such as Facebook, LinkedIn, and TV.
Many firms and executives get stuck here. There is such an emphasis on short-term results that no one is willing to invest in what it takes to make the organization successful 6 months to a year from now. Attention becomes focused solely on PPC and BD to the detriment of other channels and long-term strategy.
This results in the organization ending up in a financial hole because PPC and unsupported BD deliver CPAs that aren’t profitable. The average CPA of a PPC admission is $6,000 for in-network providers. For new BD reps, costs are $4,000-$5,000. Neither of those CPAs are sustainable when a provider only makes $4,000 to $15,000 per patient stay depending on level of care ( and that’s assuming the patient even stays the entire time, which isn’t always the case).
As organizations fall into revenue shortfalls, they again look to admissions to fix the problem. But plowing more money into PPC or BD only compounds the problem. This means there is less capital runway available for investment into longer term strategy.
For BD in particular, reputation is not just built through individual reps, but by the organization at large. When an organization repeatedly fires and hires new reps in an attempt to “reach the number in the spreadsheets”, it creates ill will in the community. Referral partners dealing with their 3rd rep in a year start to feel that the organization the rep represents is not a quality one, else why all the turnover?
The most successful reps have been with the same program for 2-3 years. So frequent turnover also disadvantages the reps. They don’t have the time they need to build, nurture, and cement the relationships that drive referrals. This goes back to our discussion about timelines. First, one has to find and train the right reps. Then they need to wait 2-3 years for them to reach optimal performance. For entering new markets where there is intense competition, double that to 4-6 years. That’s not a very attractive PE timeline for most.
Should Your Firm Invest in Behavioral Health?
This is a pretty simple answer. If your timeline for an exit is less than 10-15 years, our answer is no. Are there firms that have been widely successful on lesser timelines? Of course! But that number is, in our estimation, less than 5%. When the market was frothy and hot, people got away with a lot that would never fly today because the momentum play is gone (though many haven’t gotten that memo, surprisingly). 95% of those who have invested in behavioral health in the past 3 years have found themselves struggling to make the numbers work, burdened with a portfolio company they thought would be a home run, but is instead in need of constant attention and solutions which they don’t have the ability to provide.
Points to Remember
The market is oversaturated. Behavioral health is not a space where you “build it and they will come”
Due to oversaturation, providers must have a differentiated competitive advantage in terms of their service(s) provided
Make sure you understand What Good Looks Like in regards to the clinical delivery of your services
Be patient. Plan for a 10-15-year exit
Google Ads will not save your census. In fact, it’ll break the business financially if overly relied upon
Behavioral health is local and reputation is everything
Multistate expansion is almost never a good idea. Expand locally and regionally first
Copying what larger providers have previously done is probably the wrong strategy
Firms must think qualitatively beyond the spreadsheet. What steps with what timelines are actually needed to get those numbers to work? Go in with the assumption that you’re missing several critical steps which you’ll need to learn and then double your timelines
Have a go-to-market strategy for de novos or add-on acquisitions
What Makes an Attractive Behavioral Health Investment?
When we look at our most profitable clients, there are a number of commonalities.
Has existing licensing and in-network contracts, of course.
Is currently profitable. Sounds like a no-brainer, but we’re often surprised by how many investors buy failing enterprises with the thought that just a bit of better management can turn things around right away. If it’s not profitable now, that means the cost structure needs to be right-sized or the community reputation has to be rebuilt, neither of which is an easy or quick task. It’s rarely the case that it’s simply bringing some standard business know-how and professionalization in. The challenge is always much bigger.
Reasonable size per location based on population density and number of competitors in the area. For example, as a residential SUD provider, 100 beds is very very hard to fill, but 6 is too small to make the numbers work consistently. Investors want to find that sweet spot of not too big and not too small for the market. If the current census is regularly at 80% capacity, that’s a good indicator that they’re the right size.
Hub and spoke model offering full continuum of care. Both payers and patients, the two most important customers for any provider, want one system to access all levels of care. This also makes the spreadsheet numbers easier. A $2,000 marketing CPA is a hard pill to swallow if the patient is only doing one level of care. But if the patient does detox through IOP, that’s twice as much revenue, so much easier to work with.
Has a strong reputation in the community. It’s not just about what the current CPA is, it’s also important to qualitatively evaluate how key referral partners see the provider. Referral volume will make or break any provider.
Lower than average industry turnover. If most staff have been there for 2 years or more, that’s a great sign.
Training programs for all roles. Note, this does not mean a 1-to-2-day onboarding where they learn about payroll and the EHR. This is at least a week-long training per role that includes best practices for the role as well as a shadow period. Also, it is NOT just a shadow period. There must be some kind of standardized training that teaches all staff What Good Looks Like for their role with attendant KPIs for them to be able to measure success. Yes, this includes the clinical team.
There is a reasonable growth strategy in place. 40% YoY growth is not reasonable. It will break the org. We’ve seen it again and again. If the program has experience opening 2 new facilities a year, don’t suddenly expect them to open 6 or more the next year. It will all break. Growth should occur in stages and be mostly incremental in order to succeed. Don’t believe us, look around at the behavioral health landscape and identify how many providers exist that have grown exponentially over the past 10 years? There are none. The ones that tried are now either closed or stalled.
Multichannel marketing. Simple diversification here. No provider should be overly reliant on any single marketing channel or referral source. Too much concentration creates significant risk.
Compliance. Payer audits are very real and often come to the tune of millions of dollars in claw backs plus frozen payments for 6 months to a year as the audit is completed. There should be no shortcuts when it comes to documentation, billing, quality assurance of care delivery, etc.
Looking for help with a prospective or current acquisition? We do due diligence and exit strategy consulting with a 30-day turnaround. We also provide best-in-class, full service behavioral health marketing across online and traditional channels. Our clients include UHS, Recovery Centers of America, American Addiction Centers, Caron, CleanSlate, Community Medical Services, and Baymark to name a few. We’ve helped brand new providers successfully open their first location as well as the largest providers in the country right size and/or grow existing operations. Get in touch with us here to see how we can help you succeed.