
We’ve personally observed over 25 different programs this year alone. We’ve seen great programs and we’ve seen ones that need a lot of work. So what makes a great addiction treatment program stand out? And how does that translate into long-term organizational growth and success?
If you don’t know what our team does, we go into treatment programs across the country and get very deep into their entire organization. We dive into financials, clinical programming, org structure, leadership, marketing, business development, operations, and technical integrations. We have over a billion dollars of operational data and over $100 million of pure addiction treatment marketing data from programs as small as a million a year to the largest providers in the country doing 300 million+ in revenue.
This has given us a unique perspective where we probably have more data than anyone else in the country, but also a layer of qualitative analysis on top of that. When we go into a program, we observe their clinical programming, meet with staff, interview patients, interview alumni, walk through systems, analyze the data, etc. It gives us a real 360-degree view on a program. In this article, we’ll be sharing both some of the data as well as our qualitative insights into what makes a program successful.
It also allows us better insights into nationwide trends in the space. This article will provide an analysis into broad trends affecting the field, what opportunities we see for growth, and how successful programs are navigating those trends to their advantage.
What Are the Hallmarks of Successful Treatment Programs?
We’ll start with the basics. You must have a program that adds value where other programs don’t. A number of factors we’ve written about before allowed generic programs to thrive without differentiating. This is no longer the case.
Understanding and creating your unique value is the key to any successful organization, and it’s a hell of a lot harder than you think. The main question you need to ask here is:
“Does anybody else do that well as well?”
For example, providers often tell us, “We have great staff.” Do other people have great staff? Then it’s not a differentiator and you’ll find it much tougher to build long-term sustainability.
Other examples we often hear are: “We really care about our patients” or “We offer dual diagnosis and trauma-informed care.” Do other providers do that too? You bet!
Tons of providers offer the exact same thing, so that’s not going to help you in a crowded marketplace. In fact, we bet as you think about what you consider to be your program’s greatest assets, you’re probably a little horrified to realize that, every time you ask yourself, “Does someone else do that too,” you’re answering, “yes”. Don’t worry, most of our clients find themselves in the same spot when we first engage with them.
Now, you could get specific with these. That might help. For example, “We offer dual diagnosis treatment to LGBT individuals” or “We are the only dual diagnosis treatment provider in Erie, Indiana.” In these cases, you might be the only, or one of the few, offering such services to those communities.
If you do not have unique differentiators, then you’re probably relying on some specific referral relationships or expensive outbound marketing. However, without something truly valuable that stands apart, you’ll be susceptible to competition that comes along and does it better. This is why we continue to see small providers closing down quite frequently.
You’ll also notice in this exercise that you never once thought that, “We have the best marketing,” “our website is the most appealing,” or “we have better referral relationships than others.” That’s because those elements don’t drive long-term success, they only fan the flames of success that’s already there.
When it comes to marketing, we often like to use the example of a fire. Marketing is a lot like lighter fluid. You can pour a ton on to get things started, but that time and money goes up in flames fast unless you have good wood underneath. That good wood is your treatment program.

Of course, you could just keep pouring lighter fluid on the fire, even if the wood was bad, but you’ll run out of money pretty fast doing that, which we’ve seen happen over and over again in this field.
“We can’t market thin air,” is one of our favorite quotes. Marketing can’t make a business, it can only build upon the good product or service underneath. More importantly, as you build up the logs of your services, you need less and less lighter fluid to build it higher, which is exactly what happens. Over time, marketing costs go down when the business is built right.
It’s a big reason why we built out the consultant wing of the business – to create a foundation for success. Otherwise, you just burn that marketing money away.
Which Is Why Clinical Must Be the Center of Your Strategy
Alignment with core clinical differentiators is at the heart of every successful program we’ve worked with. You may not be surprised to learn that those struggling most are the ones that can’t articulate what they’re actually good at.
This again is a trend that has changed. You could get away with a really shoddy program for quite some time simply because there always seemed to be more patients available at the right price, whether you were pumping that money into Adwords, unbranded SEO, or affiliate marketers.
Do you know how many business development reps we’ve come across this year who had never even actually been in the facility of one of the programs they were working for? How can they possibly recommend your program if they’ve never stepped foot in a facility?
So what happens? They fall back on features. They’re trying to promote a pool, the McMansion, the master’s level clinicians, the dual diagnosis programming. What’s worse, they have no idea who to target. They talk to everybody and anybody. So maybe the people they send to your program are a good fit and maybe they’re not. The patient won’t know until they get there since the rep had no clue what the program actually entailed anyway. Same goes for your marketing and even your call team.
From your marketing to your website to the conversation on the phone, every individual needs to know what your program does the best and also who it best serves. When those two things are in alignment, magic happens.
Just think about it like an actual patient journey. Let’s use our LGBT example. The patient sees an ad promoting an LGBT specific program. They call and the rep on the phone gives them details on what sets it apart from other programs. The clinicians in the program have focused on serving the LGBT community for years now and have become incredibly good at it, better than other programs that say they have an LGBT program, but actually don’t (just a small note here: The National Center for Biotechnology Information did a study on addiction treatment programs offering LGBT services. They found that, of the 900+ facilities offering treatment programs for LGBT, only 7.4% could actually name any such specialized programming when called. Talk about false advertising!)
Because this patient got highly specialized services, their treatment was very effective. They went out and told their psychiatrist, family, friends, and others in the LGBT community about the program. They also left a great review online. In this way, by having a quality program where everyone throughout the organization communicated the same message, they attracted the right patient into the program and that patient then became an advocate for them upon completion.
THIS is what drives down marketing and admissions costs over time. The psychiatrist who refers their next LGBT patient struggling with addiction, or their colleague they recommend it to who has a similar patient, or the individual that sees the online review which gives them the confidence to pick up the phone and make a call.
This is traction and momentum. It’s what happens when every message in the organization attracts those who you can best serve. Over time, your reputation reaches a critical mass and large numbers of psychiatrists, family members, community partners, and those in the LGBT community not only know who you are, but trust that you do what you say you do well.
Now imagine if that entire chain had worked, except, when they got to the facility, there wasn’t actually any special LGBT program, like the 93.6% of providers in the NCBI study. In this case, all that marketing spend that went into admitting that patient has zero extra tied to it. In fact, that individual may actually leave a negative review and say bad things to all the same potential referral partners. So now it’ll cost you at least the same amount, and maybe more of your marketing budget to connect with the next patient.
And, let’s be honest here, it’s no secret that even some of the most well-regarded programs in the country were using duplicitous marketing tactics such as paying affiliates for calls, buying flights, or using hundreds of unbranded sites to drive volume. Many older programs in the country were just as undifferentiated as the newer programs popping up in the typical hot spots, completely dependent on callers who didn’t even know who they were finally on the phone with an admissions rep.
What Does Good Clinical Look Like?
You may be surprised that a lot of programs don’t know. There has been a strong tendency in the field, even among more respected providers, to allow for a vast array of eclectic therapy with little oversight. We’ve come a long way regarding our knowledge of addiction treatment, what works and what doesn’t, in the past 50 years. But you may be hard pressed to see some of that knowledge and research incorporated into modern treatment.
Great clinical programming is about skill building, something most clinicians, through no fault of their own, are not taught in school. They learn a lot of theory, and are very comfortable running lecture-style or psychoeducation groups. But one can’t learn to ride a bike by listening to lectures about bike riding. You need to get on and ride.
Finding recovery is the same. Skills sets must be practiced until the neurological pathways are built up and automated, unconscious processes become habit. Setting skill building objectives in private and group sessions, then having patients practice is one of the best ways to foster long-term recovery that lasts even once they leave treatment.
For the same reason, maximizing patient involvement and engagement is critical. The more practice they get, the better. Have you ever sat in a group where the therapist went around the circle and asked patients questions 1 by 1? Us too. It’s the most common style of group facilitation. But it’s far from the best use of time.
With just 10 people in group, the 1 by 1 facilitation means that a single group member gets a maximum of 6 minutes an hour to practice new skills. Even at 8 hours of group time a day, that’d be less than 1 hour total per day!
Maximizing clinical efficacy in a group setting requires regular methods of full group involvement, pair work, and small group work. Remember, in these settings, just listening doesn’t truly count as involvement. Listening to others about bike riding is only minimally beneficial to learning how to ride yourself.
Excellent programs have skills-based objectives for individual and group sessions. They also facilitate group in such a way that that skill set practice is maximized.
Budgets Aren’t What They Used to Be
For a long time, many programs were comfortable paying high acquisition costs for new patients. The reimbursements were high enough and competition was low enough that reputation didn’t matter that much. Lowering marketing and admission’s costs weren’t a priority since they’d inevitably be covered.
Additionally, a small percentage of addiction calls are always crisis calls, people looking for treatment right now. Those calls are pretty easy to admit on the phone, as they’re desperate for treatment immediately. But that’s not the majority of people calling in, and untrained call reps fail more often than not when connecting with someone more discerning. Especially with all the bad publicity the field has had, potential patients and their loved ones are more cautious than ever.
But we all know that no program can operate like that anymore if they want to survive until next year. Most treatment programs considered a 2-3% call to admission ratio good, but that’s actually terrible. That’s why we strive to help client’s phone admissions teams get into the 5-10% range. Training, systemetized follow-up, and highly targeted marketing are all part of that equation. Additionally, if you built your reputation right, many callers have decided to use you before they call. It’s a hell of a lot easier for a rep to admit someone already convinced of your program than someone who called off a single random Google ad or 1 landing page visit.
So many programs stayed out-of-network for the same reason of high reimbursement. The reimbursements were so high that you could afford to turn away an additional 90% of potential admissions. Nowadays, that’s rarely the case. If you want to be a pure out-of-network provider, you have to become better than ever at differentiating your reputation and highly targeting your marketing, like we discussed above.
Successful programs these days integrate their marketing channels to build traction and momentum, thereby reducing costs per admission over time.
Who’s more likely to get in the door with a potential referral partner, the business development rep that cold calls with no marketing support, or the one that calls where the referral partner has seen the provider over and over again across advertising channels?
If a patient does a Google search for treatment, are they more likely to click on the provider they never heard of in position 1 or the one they kept seeing on Facebook showing up now in position 2?
These answers are obvious. Just marketing across two channels, like SEO and Facebook in our example above, are more cost effective than putting the entire budget into just one of them.
As you can see below in this example where we track Assisted Conversions for a client, even with Adwords paid search, a full 22% of conversions from that channel were actually assists, meaning that they first landed on the website from Adwords, but ended up calling after arriving at the site again from another channel like Facebook or organic search.
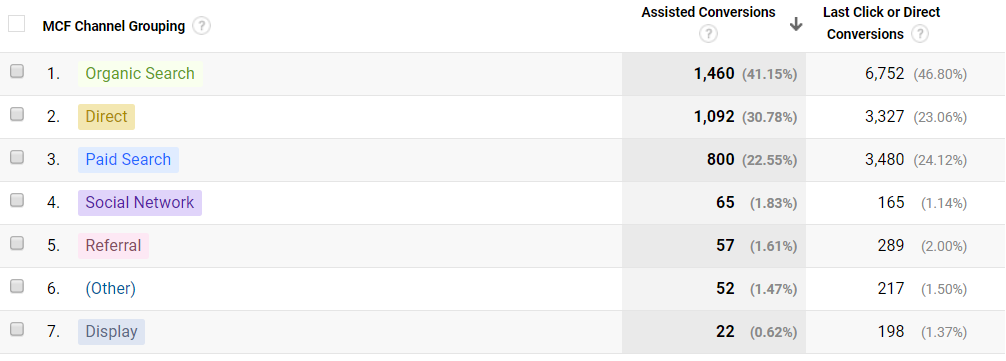
So if you’re only tracking final attribution, meaning you only track the final page or the final channel a person called from, you’re doing it wrong.
This one really isn’t a trend. Unlike other areas of healthcare, we simply don’t see a lot of sophistication in tracking or integration across multiple channels. The SEO agency doesn’t talk to the Call Team who doesn’t talk to the BD reps, none of who talk to the people actually running the program. Sometimes the simple act of setting up cross functional meetings with our clients can drive a world of change.
You would not believe how much money we find simply going into black holes. Often just compiling the existing data, you can find hundreds of thousands of dollars lost to poor marketing, clinicians discharging patients early, improper billing, poor clinical documentation, duplicated or redundant processes, etc. We’ve gone in and tripled client revenue in a month sometimes just by highlighting existing processes or staff actions that are costing the program ridiculous amounts of money. We have one client that we saved them over $7 million in our first year working with them just be identifying extensive redundancies, lost opportunities, and extraneous costs in the initial engagement.
Knowing what to track is the first step in gaining a handle on your organization’s overall health and sustainability.
Don’t Chase Reimbursements
Have you ever noticed that mostly programs that grew to a large size, the ones most people know, were/are spread out all over the country? Did you also notice how many failed or are struggling now? You may remember Sovereign’s strategy. Whenever their losses were becoming unsustainable, they’d go out and raise capital for a new center, then use that money to pay off the previous debt, always one investment ahead of bankruptcy, until they weren’t.
There are still providers out there like that, ones that look like they’re growing on the outside, but are struggling to stay solvent every day.
This is because a national model is really, really difficult to manage. You have money and resources spread across wide geographical areas. There is also no synergy between the programs. They can’t really feed into each other, especially now that so many fewer people are willing to travel for treatment than just a couple years ago.
We’ve seen providers, particularly in hotspots like Orange County, Prescott, and South Florida, go chasing after good policies. Maybe they do this in terms of geo-targeted marketing spend, strategically placed business development reps, or by finding a referral contact with good policies. And what happens every time?
A red flag goes up at the insurance provider and they renegotiate the contract the following year, eliminating the high reimbursement. Suddenly, providers are left scrambling to find the next “good policy.” That’s no way to do business and many providers collapse before they find the next one. Long-distance marketing is always 2-3 times more costly than focused marketing spends closer to home. It’s very hard to be sustainable.
This was also the logic behind purchasing facilities across the country. The thinking went that you could simply find good reimbursing policies and have them fly to treatment. But that clearly turned out to be a short-term trend reliant on free flights, lack of local services, and high reimbursements.
Learn Local, Build to Need
Nowadays, the most successful treatment providers are the ones growing smart, growing locally and regionally.
This is one of the most important strategies to be following right now. Looking across all of our clients big and small, we can’t name a single one where we’d point to a broadly dispersed facility base as being an asset. Again, it’s not that you can’t make it work, because we have clients that are making it work, but it’s much more difficult than a more regionalized model.
Look to providers like Pinnacle, Pyramid, Granite Recovery and others with discipline and patience driving their success. They also do an excellent job of offering a large and very broad continuum of care. This drives efficiency in inquiry volume. Because their marketing is targeted to the regions they operate in, they’re in-network will all relevant payors, and they have a broad continuum of care. They have the potential to admit nearly 100% of their inquiry volume. That’s a big deal.
That often means switching from a low-volume, high margin model to more of a mixed model that includes a lot more high volume, low margin. But it’s a strategy that works today AND will work 5 years from now.
Additionally, if you talk to executives at these providers, you’ll learn how they go in and examine both community AND payor need. Rather than forcing or trying to educate the community and payors on what the provider has, they create programs that align with needs. And, obviously, a big need is quality providers in the community’s area.
There will always be room for the destination rehab model, but we see very clearly in the data that most of those calling for treatment are looking locally. Even when we have clients with call volume coming from across the nation, a majority of actual admissions still come from closer to the facility.
There are, of course, your 30-bed and smaller facilities that might survive off of a key referral relationship or two somewhere far from their actual location. Or maybe they’re paying the new brand of patient brokers that try to contract on monthly salaries in order to skirt laws. But those facilities won’t be around 2 years from now, so don’t really matter in the larger scheme of things.
And, as payors push for more outpatient models of care, localization will become ever more important.
Even in the high-cost Adwords arena, we’ve helped clients bring cost per admission down from $15,000 to under $4,000 by helping them localize spend, among other optimizations. For really local spends in non-competitive areas, and with extensive in-network contracts, we can get CPAs as low as $1,500.
Just a simple heat map of qualified call volume can give you real insight into where your calls and admissions come from, like in the below from a client in Colorado
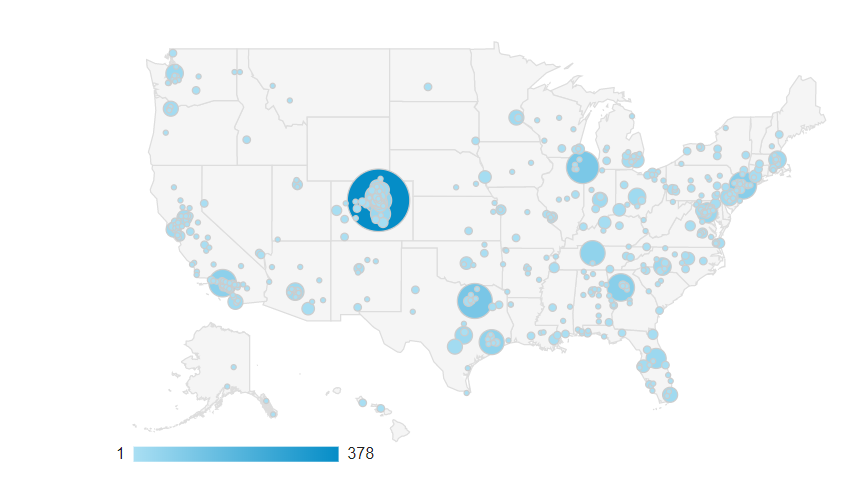
Successful programs use their existing data to determine what’s already working and to focus their marketing and growth efforts appropriately.
Data mining and analysis, not just of nationwide data, but your own data is another unrealized opportunity trend for many providers. In fact, as we often tell clients, nationwide data is not nearly as important as your own. This is probably one of the biggest mistakes we see smaller providers who are trying to grow make.
They think if they can copy the strategies or get the data from a competitor, that it’ll lead to their own success. You wouldn’t believe how many times we’ve gone into an Adwords account just to see copy pasted campaigns (with cost per calls of $1,000 or more!) And don’t get us started on the number of providers now adding an EMT track. As we always say, if all every little coffee shop in the country had to do was copy Starbucks, they’d all be multinationals with billions in revenue.
Business growth is about strategy, not tactics. It’s a game of chess. You can’t copy the moves of your opponent and win. You can’t use the same moves every single game and expect to win either. Success depends on strategically adapting to each move in the game as it happens.

This is why we have to craft a unique strategy for every client we work with. There is no plug and play or one-size-fits-all. Frankly, that’s why people hire us, because we don’t just come with proven tactics, we come with strategic insight and an ability to adapt that is what actually drives success for our clients.
What the Payors Want
The payors want to reduce costs. No surprise there. They’re looking to deliver quality treatment at the lowest cost. The reality is that they have no problem testing this. If they cut a few days off of what they provide for PHP, for example, and they see no change in outcomes for patients, then that tells them that PHP with less days is just as effective.
This is just one more reason why tracking internal data is so crucial. If you can prove your case that providing 20 days of PHP instead of 15 leads to better outcomes with your treatment model, then payors are much more likely to approve treatment. But if you have no data, you’re SOL. Our clients with the most success negotiating better reimbursement and more days have lots of internal data. We know one provider in PA that has never gotten denied a UR extension in over a decade because their data and documentation is so robust.
While providers prefer higher reimbursements, hence the desire to build residential facilities or other high levels of care, this trend is continuing to decline. If you want to be here five years from now, you need to build outpatient programming into your model. Just like with destination rehab, a small number of high-cost, high level of care facilities will survive, but many will be pushed to the wayside.
The provider/payor relationship can sometimes be adversarial, but nobody wins in that game. Actually, that’s not true. The payor wins most of the time. Addiction treatment is a tiny part of overall healthcare, and the payors are bigger than the biggest healthcare system. Like it or not, our most successful clients work with the payors, not against them. This gets them higher reimbursement rates and fewer expensive billing or UR issues.
And the payors have told us and our clients again and again that their goals are high quality care that gets results at reasonable rates. That’s a tough spot to be in. Payors want you to provide higher quality while doing so for less. Then again, it’s a pretty natural market force present in every sector of the economy, so nothing new.
That means really efficient operations, sophisticated marketing that doesn’t result in excessive cost per admits, outcomes data to prove efficacy, and maintaining an excellent team that can deliver on all of that. Certainly a tall order, but some providers are already stepping up to the plate. If you’re not willing to compete in that arena, the road ahead will be a tough one.
Hire, Fire, or Train, the Choice Is Yours
A strong business development team has always been part of our strategic marketing plan for clients, so it’s no surprise that this team still accounts for the majority of admissions at a reasonable expense.
The problem here is that most business development reps have received no training, even if they’ve been in the field 10+ years. Most also are only comfortable collaborating with other treatment programs. It’s the easiest form of outreach, but it’s also the form least likely to build long-term viability.
Case in point, most programs we go into have reps only bringing in 0-3 admissions a month these days. Our clients with well-trained teams are still helping 8 or more people a month get into treatment. This is one of the key reasons we’ve been building out onboarding programs for our clients’ business development and community outreach teams. We’ve seen the huge impact a well-trained team has on results.
Instead of training, most programs are still hiring and firing in rapid succession. On LinkedIn, it feels like we see some reps changing treatment centers every month. Providers are still looking for that magic bullet – the “book of business” – which has never worked well long-term, and usually not short-term either.
Both successful providers and successful reps know how to network across a wide range of referral partners, but in a strategic way. They don’t just go out and do 15 face to face meetings a week because that’s the output KPI the Director of Business Development set. Similar to our discussion of focused effort at the beginning, great reps know what the differentiators of the facilities are and who’s most likely to benefit from that unique value. They meet and spend time with the right people.
A well-trained BD team also combines with internal data tracking and strong clinical programming. Your reps can use this in meetings with knowledgeable referral partners who are looking for proof of quality care before sending anyone to you. Again, it’s all about how you integrate and align teams across the organization.
We’re happy to say there is an overall trend towards better training and organizational alignment across quality providers. When we added the consulting wing of the business onto our existing marketing agency, we only had a handful of clients take advantage last year. This year, we’ve been non-stop busy with the consulting end of things. You also get to meet great teams of people who really care. Because only providers really focused on driving growth while focused on quality care are the ones willing to invest in themselves and their teams in that way.
Where Does MAT Fit In?
This has been a trend for a while. What we’re finally just starting to see is an integration of MAT into the traditional rehab model. Before, Methadone clinics, Suboxone providers, and traditional Detox to IOP kept this very separate.
The recent trend, and it’s very recent, is to provide both, and this is the future of treatment we’re seeing. There will remain an ever decreasing demand for specific treatment options. The future is integration.
We’re seeing more and more payors deny detox or even sometimes res for OUD patients due to the cost effectiveness of MAT. On the other hand, MAT in its weakest form, where patients just get a script and 15-minute behavioral health check-ins, also isn’t viable long-term.
What’s happening, and needs to continue to happen, is differentiated care where patients that can benefit from an MAT protocol are assigned one alongside traditional therapy. Treatment has never been one-size-fits-all, and that remains the case when looking at incorporating MAT.
From a business standpoint, the land grab continues with the biggest players in the space, such as CleanSlate. Right now, it’s possible to open up a facility and fill it in under a year due to high demand and no competition.
This was exactly what we saw with traditional rehabs 10 years ago or what we see in Dermatology today. You could hang a shingle and immediately fill beds because demand was greater than supply.
However, just like traditional rehabs got a jolt of surprise when the market got saturated, the same thing will happen to MAT providers. Competition is already heavy in some markets, and we give it 2-3 years until competition for the MAT clinic model also reaches a saturation point where more sophisticated care delivery and marketing models will be required to be sustainable.
Wrapping Up 2019 and Looking Forward to 2020
Key Trends:
- Uniquely focused clinical quality as a primary differentiator in highly competitive field.
- Continuing push from payors to move to outpatient or lower cost models of treatment. Continued preference for in-network contracts with climbing deductibles or co-insurance on PPO plans.
- Overall consumer preference for treatment closer to home. This is also connected to a lingering distrust of the field overall due to bad publicity and bad experiences.
- Increasing competition. While many programs have closed, we’ve seen just as many new ones pop up.
- MAT will continue to be in-demand as a low-cost option from payors, but will need stronger integration with traditional behavioral health interventions.
Key Opportunities
- Clinical programming that breaks the current mold and focuses on skill-building and recovery capital.
- Sophisticated tracking of clinical outcomes that can be used to prove necessity and efficacy to payors as well as consumers.
- Locally and regionally relevant programming.
- Integration and alignment of all business units along core values and unique program differentiators. This must also be integrated in marketing messages across channels.
- Build out of internal training processes to develop highly skilled teams.
- Build out of internal tracking across business units and marketing channels to capture cross unit and cross channel interplays.
Key Pitfalls
- Geographically dispersed facilities across the entire US.
- High-cost marketing and unbranded marketing.
- Lack of alignment across the org.
- Untrained teams.
- Chasing higher than average reimbursement rates.
- No tracking, poor tracking, or messy data.